Colorado Charts Its Own Course on Vaccines Amid Federal Pullback
This article, which originally appeared in KFF Health News, features SE2’s Elizabet Garcia and highlights the Colorado Chooses Vaccines coalition, which SE2 helped create. SE2 also provided communications support for the coalition.
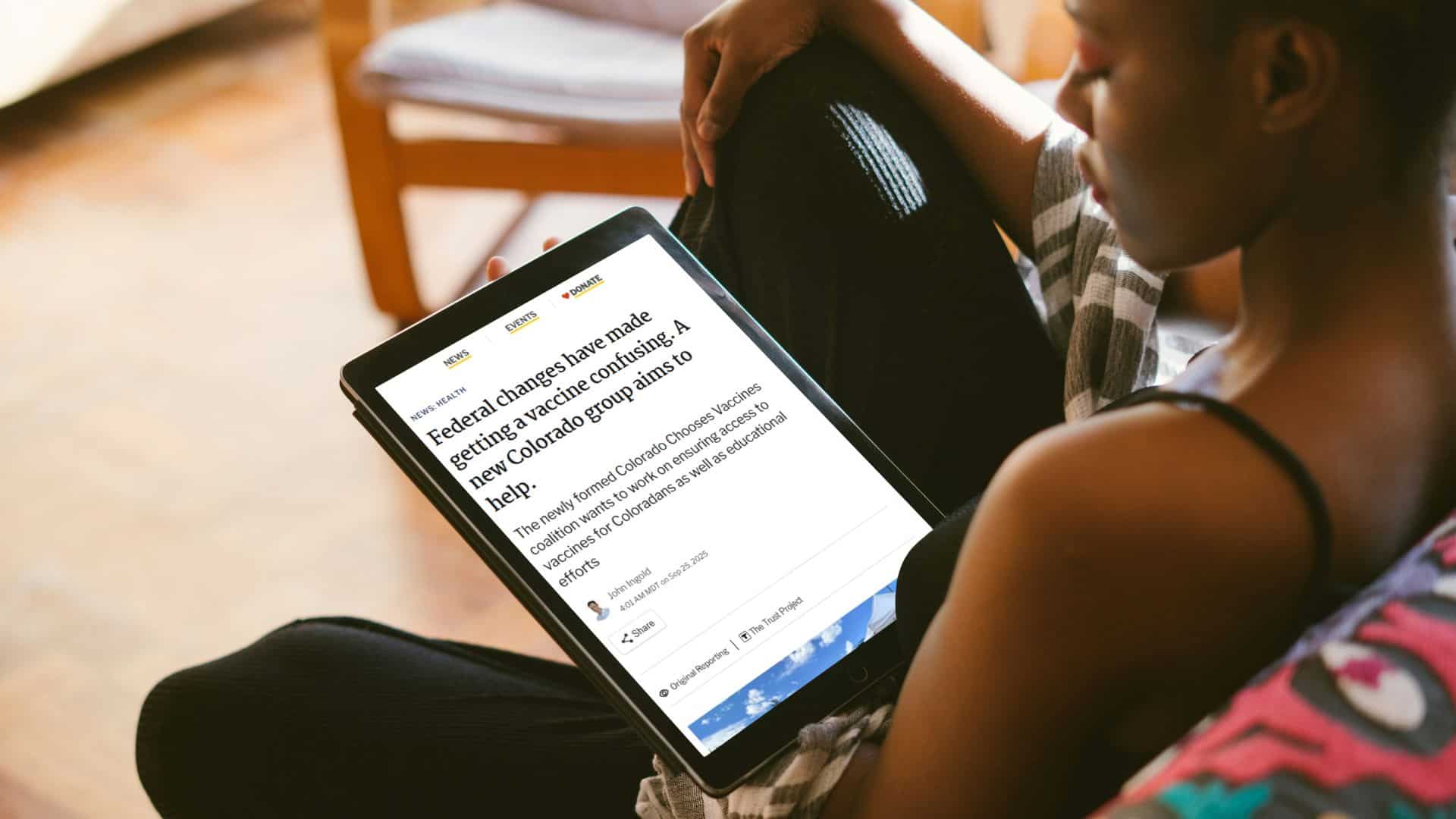
In response to abrupt and politicized changes to federal vaccine policy, concerned Coloradans have taken several steps to shore up support for vaccine science.
A bill passed by the state legislature in March then signed into law by Democratic Gov. Jared Polis allows Colorado to further uncouple itself from federal guidance.
The law allows health officials to follow the recommendations of national medical groups when making decisions such as purchasing bulk vaccines for the Medicaid program.
“We are insulating our state from the dysfunction coming out of Washington,” said Democratic state Sen. Kyle Mullica, a co-sponsor of the bill and a registered nurse. “We’re going to rely on science.”
“From fighting during the pandemic for Coloradans to get vaccines as quickly as possible to combating the Trump Administration’s barriers to getting vaccinated, we have expanded access to vaccines for Coloradans who want them,” Polis said in a statement when he signed the law.
Colorado is one of at least 29 states that, along with Washington, D.C., have taken steps to bypass the new federal recommendations amid worries that the changes could chip away at public trust in vaccines and erode broad vaccine coverage.
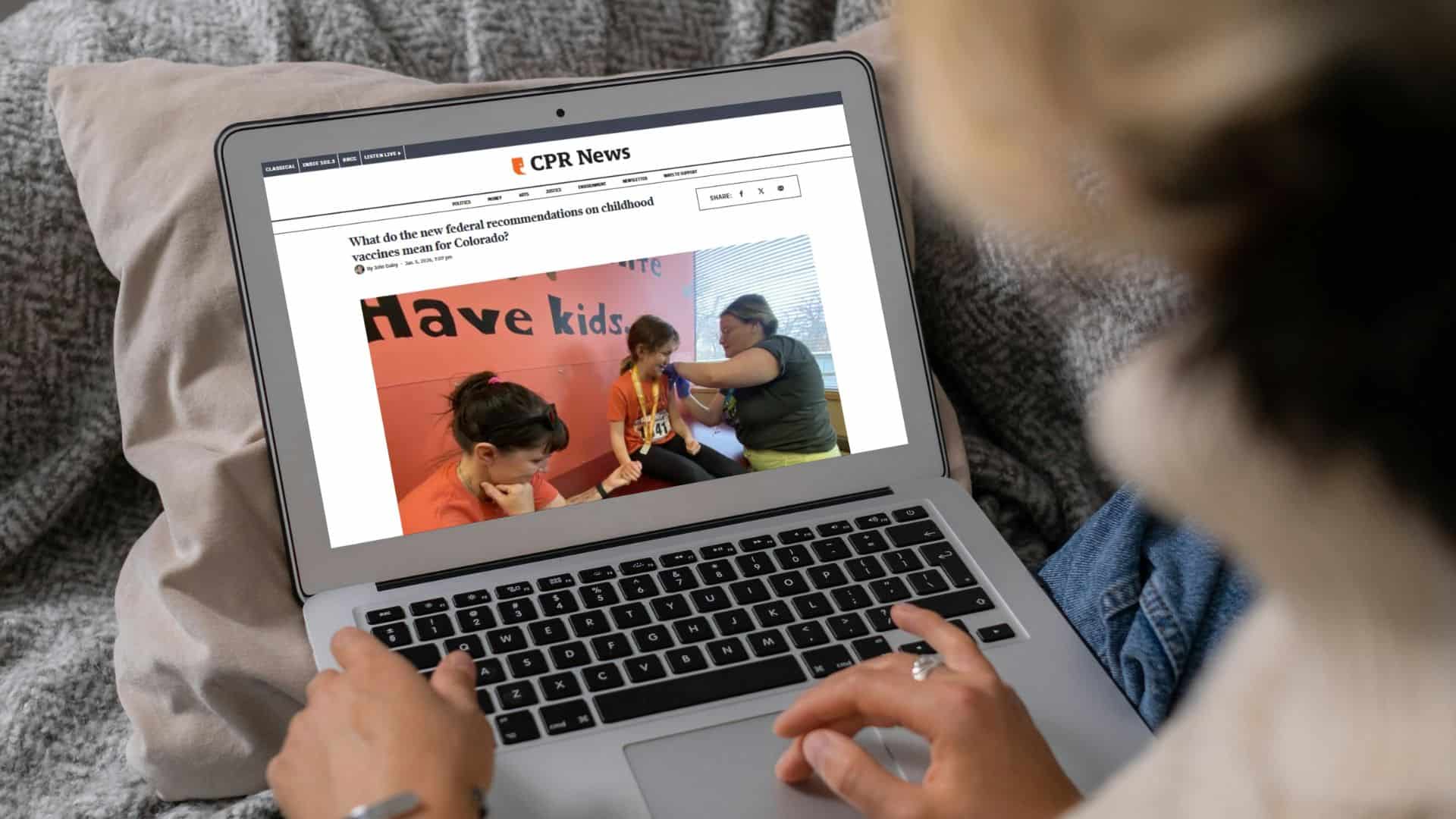
Previously, Colorado, like most states, had followed federal guidance set by the Centers for Disease Control and Prevention. In January, CDC advisory panelists, selected by Health and Human Services Secretary Robert F. Kennedy Jr., removed six pediatric immunizations from the agency’s universal recommendation list.
Last year, doctors, scientists, local leaders, and other supporters came together to form an outreach and advocacy coalition called Colorado Chooses Vaccines.
The group aims to offer a clear, unified voice on the proven benefits of vaccines and reassure residents confused by the many federal changes.
Carol Boigon, a former Denver City Council member, joined the group because she wants more people to hear her own chilling story about vaccine-preventable illness.
“Every summer everybody got sick,” Boigon said, recounting her childhood in 1950s Detroit.
The illness was polio, a highly contagious viral disease that attacks the nervous system, sometimes causing partial or full paralysis.
During the summer of 1953, “the whole block was sick and some of us got crippled, and that was just the way it was,” she said.
New Group Steps Up
Boigon’s personal history will be part of the coalition’s work to educate new generations about the dangers of infectious diseases that were once common in the U.S. but are now relatively rare.
The group, which formed last September, will also compile vaccine information from medical groups and the state health department and advocate for policy proposals with the state government.
Several pieces of paper are arranged on a table. One is a professional biography of Carol Boigon from the Denver City Council. Next is a clipping from The Detroit Times. Last is a 1985 Colorado Press Award.
Boigon shows memorabilia from her life and career. (Kevin J. Beaty/Colorado Public Radio/Denverite)
“It was in direct response to the federal threats,” said another coalition member, former state lawmaker Susan Lontine. She leads the nonprofit Immunize Colorado.
Another member, public relations specialist Elizabet Garcia, wants more outreach to Hispanics, whose vaccination rates lag behind other groups’.
“A lot of time it’s this fear that they’re going to have to pay out-of-pocket, that their insurance doesn’t cover it, that they might not even have insurance in general,” Garcia said.
Boigon was 5 when she got sick and was hospitalized for six weeks with a fever. The virus attacked her spine.
“None of my limbs worked immediately afterwards,” Boigon said.
Although she regained function in her other limbs, her right arm never fully recovered. She had to adapt, relearning everyday tasks such as reaching out to shake hands with people with her left hand.
In 1955, not long after she got sick, the new polio vaccine became more widely available to the public. As vaccinations took off, U.S. cases of polio, once one of the nation’s most feared diseases, dropped by an estimated 85%-90%.
Increasing Public Trust
State leaders have taken other steps to promote public health. After the Trump administration pulled the U.S. out of the World Health Organization, several states, including Colorado, decided to join the WHO’s Global Outbreak Alert and Response Network on their own.
Colorado also joined a multistate lawsuit challenging the Trump administration’s changes to the childhood vaccine schedule.
And the new state law has provisions besides allowing the state to diverge from federal recommendations. It codifies pharmacists’ ability to prescribe and give vaccines themselves. It also increases legal protections for healthcare workers who give vaccines.
“This law will provide more clarity to guide all Coloradans, including providers who administer vaccines,” Lontine said.
But the legislation has opponents who say it would interfere with parental choice and claim vaccines might be unsafe or ineffective.
“I just want to make sure we’re not just getting into a big political dispute between the federal recommendations — the CDC and so forth — and different political views in Colorado here,” said Republican state Sen. John Carson, who voted against the vaccine bill.
NPR contacted the U.S. Department of Health and Human Services about Colorado’s new law. Spokesperson Emily Hilliard answered in an email: “The updated CDC childhood schedule continues to protect children against serious diseases.”
Preventable Illnesses Surge
The flurry of statewide activity comes as Colorado and the nation have seen surges in illnesses such as flu and measles.
As of mid-May, Colorado had recorded 22 measles cases this year. In 2025, it registered 36 cases, according to the state health department, far surpassing totals from previous years.
Across Colorado, kindergarten vaccination rates for measles were 88% last school year — with only a few counties achieving rates of 95%, the level needed for herd immunity, according to data published by The Washington Post in December.
This has also been Colorado’s worst flu season in recent years.
Vaccination rates for both flu and covid-19 have dropped slightly in Colorado, according to the state health department.
Eight children in Colorado have died this season from flu; one from covid; and one from RSV, or respiratory syncytial virus. Vaccines for all three are available for children and recommended by the state’s health department.
Kennedy, a longtime anti-vaccine activist, has defended his decisions to overhaul the recommended schedule for childhood vaccinations.
In March, a federal judge put on hold many of the changes.
“We’re not taking vaccines away from anybody. If you want to get the vaccine, you could get it. It’s going to be fully covered by insurance just like it was before,” Kennedy told CBS News in January.
When a reporter suggested the new changes could result in fewer people getting a flu vaccine, Kennedy said: “Well, that may be, and maybe that’s a better thing.”
Boigon is sometimes incredulous at everything that has happened.
“It’s like we’re going backwards,” she said. “It’s like we have decided we don’t want a modern life; we want to be back in the 1950s, where children are sick and dying.”
This article is from a partnership with Colorado Public Radio and NPR.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.

Public Health Is Losing the Vaccine Narrative. Here’s How to Take It Back.
Immunization misinformation is eroding trust in health institutions and in vaccines, leading to outbreaks of preventable disease, unnecessary hospitalizations, and death.
Inaccurate information is filling a vacuum with a clear, though misleading, story that is increasing vaccine skepticism.
Federal budget cuts have reduced vaccine promotion nationwide. Many state and local public health agencies now operate with fewer staff and fewer resources to run sustained, science-based vaccine promotion campaigns.
Public health officials are under pressure to be more muted about vaccines. Political leaders try to walk rhetorical tightropes. Institutions and advocates are just plain tired.
Media now report that Washington federal health officials, including Health and Human Services Secretary Robert F. Kennedy Jr., have been told to ease up on anti-vaccine messaging to boost Republicans’ chances in mid-term elections. It’s a tempting moment for vaccine advocates to take a breather. That would be a mistake.
This is not the moment to pause, but to build a better vaccine story.
When the health sector pulls back, misinformation moves in. It keeps telling the same story with clarity and repetition. It fills the space with claims about freedom, risk, and distrust. It gives people a language to explain their frustration with institutions and politics.
That is how narrative power works, regardless of the facts.
A narrative is not a single message. It is a pattern people absorb over time. It shapes how they understand what is happening, who is responsible, and what they should do.
Right now, a negative pattern is forming without enough counterweight.
Vaccine advocates have tried to respond with science. That matters but it can’t compete with the vivid anecdotes people hear from neighbors, social feeds, and prominent vaccine skeptics every day.
If advocates are waiting for public health agencies to lead a new vaccine narrative, they will be waiting in vain.
This next phase belongs to the broader network that shapes how people understand health every day, like clinics, schools, employers, community organizations, faith leaders, local media, and advocacy groups.
These people have the reach, trust, and flexibility needed.
But we must move strategically.
Vaccine misinformation has evolved so that it can spread more widely.
It says your health is your choice, institutions don’t tell the truth, strong parents question authority, and refusal = agency. Who could argue with this?
Public health still answers that story as if it were a technical error—sending data, issuing guidance, correcting claims.
The real problem is not a lack of information. It is a gap in meaning.
People make vaccine decisions based on the realities of their lives. They think about whether they can miss work. Whether the clinic is open when they are free. Whether they felt respected the last time they sought care. Whether a vaccine itself has ever made them feel under the weather. Whether the rules seem to keep changing. Whether anyone in power seems to understand their daily life.
Those experiences shape the stories people tell, and those stories become the narrative.
If you want to rebuild confidence, you have to show how health decisions are shaped by the conditions people live in every day. Access. Cost. Time. Trust. Stability. These are not side issues. They are the experiences people use to decide what is credible.
Advocates must step out of a reactive mode, where they wait for the next false claim or political flashpoint. They can use this period of relative quiet on the federal front to build a stronger narrative before the noise returns.
A better story starts with a clearer and more straightforward frame.
Vaccination helps your child stay in school and allows you to go to work, so your family doesn’t lose income. Getting your vaccines protects your loved ones who may be more vulnerable to disease because they’re very young, older, or have chronic health conditions.
This narrative aligns with values people already hold. Stability. Care for family. The freedom that comes from not being knocked off course by preventable illness.
Advocates are not bound by the same constraints as public agencies. They can speak more freely, move faster, and coordinate across sectors. They can test and repeat messages in real time.
But that requires discipline.
- Move from waiting for the next crisis to leading.
- Use trusted voices outside of public health.
- Tell stories grounded in relatable experiences. Show how people navigate work, school, and family decisions.
- Make action easy and visible. Say where to go, what it costs, and what to expect, removing friction.
- Stay consistent. Overarching narratives shift through repetition across settings and over time.
This is not about saying more. It is about filling a vacuum with a better story.
Right now, misinformation is doing that work and it’s winning.
If advocates step in now with a clear, consistent narrative rooted in how people experience health, they can shape what people believe before the next wave of federal political messaging takes over.
If we wait, we will be back in reactive mode, trying to catch up to a story that has already hardened.
This is the opening to tell a better story.

The Barrier to Support Line Use Isn’t Just Stigma – It’s Our Tendency to Over-Sanitize the Experience
For years, we have treated stigma as the primary barrier to using support lines. We have built campaigns to normalize help-seeking, reduce shame, and encourage people to take that first step.
And yet, hesitation persists.
We may have been solving the wrong problem.
When people pause, it is not because they feel judged. It is because they are worried about what will happen next.
What People Are Trying to Figure Out
When someone considers reaching out, the questions are not abstract. They are practical and immediate: Is this free? Is it confidential? Who answers. Is it a real person? What happens after I start? Can I get out of it? Will this create unintended consequences?
Those questions are shaped by more than the moment itself. They are shaped by the broader environment we all face every day.
We are accustomed to subscriptions that are hard to cancel, services that overpromise and underdeliver, hidden fees, and systems that escalate our commitment once we enter them. We all have learned from experience to be cautious.
So when users encounter a support line, they do not assume it is simple and contained. They assume it comes with strings attached or hard-to-spot fine print or catches.
At that point, the decision is not about whether help is needed. It is about whether the experience feels safe enough to try.
Where Behavior Breaks Down
In behavior change, uncertainty is not a minor barrier. It is often the deciding one.
When people cannot predict what will happen next, they default to protecting themselves. Behavioral research shows that people weigh potential losses more heavily than gains. When the outcome is unclear, the perceived downside expands, even if the actual risk is low and the potential benefits are high.
Ambiguity also increases cognitive load. The brain has to simulate possible outcomes without enough information. Especially in emotionally charged moments, that extra effort may be enough to stop action. So people pause. They delay. They tell themselves they will come back later. Many may not.
From the outside, this looks like people are afraid of the stigma and judgment that come with seeking support. In reality, this hesitation is largely driven by uncertainty.
The Gap We Miss
The modern approach to driving support line usage has largely focused on reducing stigma. We normalize help-seeking. We reinforce that people are not alone. Those messages are important, but they do not resolve the core issue: People are not just asking whether it is acceptable to reach out. They are trying to understand what they are stepping into.
If that question goes unanswered, they answer it themselves. And the brain tends to fill in gaps with worst-case scenarios. The interaction may escalate. It may feel out of their control. It may require more than they are ready to give. It may backfire on them.
None of that has to be true to influence behavior. It only has to be believed.
What Actually Moves People to Action
In our work with support and cessation lines, the most effective changes have not been about persuasion. They have been about clarity.
When people can see what the first interaction looks like, engagement increases. When expectations are clear, perceived risk drops. When the experience feels bounded and predictable, people are more willing to take the first step.
What is often missing is not awareness, but clarity. And clarity is not only about adding information, but also about removing ambiguity.
- Show a sample interaction, not a polished description.
- Let people see how it begins, how it sounds, and how contained it is.
- Make clear what will not happen: No sign-ups. No pressure. No loss of control.
Realism Builds Trust
One way to reduce uncertainty is to make the human on the other side feel real.
This is often approached as a branding exercise, with stock imagery or generic descriptions of trained counselors. That does little to build trust. Rather, we have seen and heard from potential users – through surveys and focus groups – that it creates distance.
What people are trying to assess is not credentials. It is the authentic nature of the interaction.
Real conversations are not polished. They start unevenly. People hesitate, backtrack, and figure out what they want to say as they go. When we only show the ideal version of the interaction, it can feel like something they have to perform correctly.
What builds confidence is seeing that the experience can accommodate uncertainty.
A conversation that starts with “I am not sure why I am reaching out” is more relatable than one that begins with clarity and intent. It signals that people can enter the interaction as they are, not as they think they should be.
That shift reduces pressure and makes the step feel more accessible.
Redefine the First Step
Another common barrier is how the first interaction is framed.
Many support lines unintentionally position engagement as the beginning of a process. Even subtle, even well-intentioned cues can make it feel like a commitment. For someone who is unsure, that is enough to stop them.
A more effective approach is to define the first step as contained and reversible. A single conversation. An opportunity to ask a question. A way to explore without obligation.
This reframing reduces perceived risk and aligns with how people actually approach change.
A Different Way to Think About the Problem
If we want more people to use support lines, we need to expand the question we are asking. It is not just about making this feel more acceptable, but about making it more understandable.
Because when people understand what will happen, the first step seems smaller And smaller steps are the ones people are more likely to take.

Filling the Federal Vaccine Information Void
The Challenge
Federal disruption and widespread vaccine disinformation created confusion about vaccine safety, effectiveness, and access. As national vaccine policy and messaging became confused, Coloradans needed a credible, coordinated source of science-based information. SE2 helped create the Colorado Chooses Vaccines coalition to fill that gap with trusted voices, public education, policy support, and rapid response to federal changes that could undermine vaccine confidence and access.
Our Approach
SE2 supported Colorado Chooses Vaccines in building a clear, unified communications platform for healthcare providers, public health leaders, community organizations, and advocates. The work centered on making credible vaccine information easy to find, understand, and share.
Key elements included:
- Coalition messaging and rapid response: Helping partners respond quickly to federal actions and disinformation with consistent, fact-based messages from trusted sources, including physicians.
- Media outreach: Elevating coalition experts and shaping coverage (in Spanish and English) about Colorado’s response to federal vaccine changes.
- Public education: Supporting CoChoosesVaccines.org as a trusted resource hub featuring medical information and reliable guidance amid conflicting national messages.
- Advocacy support: Supportive messaging in news and opinion coverage bolstered coalition-backed legislation that supported Colorado vaccine access.
- Coalition promotion: Helping demonstrate the breadth of support behind vaccine access and public trust.
The Impact
Colorado Chooses Vaccines quickly became a visible, trusted voice and a national model for how states can lead on this issue. Colorado’s independent, proactive approach to protecting vaccine access and confidence drew national coverage from major outlets, including PBS NewsHour, NBC News, KFF Health News, and NPR, as well as a stream of local coverage directly addressing Coloradans’ need for accurate, trustworthy information.
- 236 media reports placed or influenced with a total reach of 278 million impressions and advertising value equivalent to $2.57 million.
- Average website engagement of 3:24, exceeding the 2:58 benchmark for health websites.
- A broad statewide coalition of healthcare, public health, and community organizations aligned around vaccine access and trust.
Together, these efforts helped Colorado Chooses Vaccines fill a critical information void, reinforce public trust in science-supported vaccines, and mobilize a statewide network prepared to respond to shifting federal policy and ongoing misinformation.